Vera A. Orlova1, Irina I. Mikhailova1, Vitalij L. Minutko2 and Irina N. Malisheva3
- The Moscow Research Institute of Psychiatry - Affiliated Office of Federal Medical Research Center of Psychiatry and Narcology, The Ministry of health, Russian Federation, Poteschnaja, 3, 107076, Moscow, Russia.
- Mental Health Clinic, Leninsky prosp., 158, Moscow, Russia.
- Modern Medical Technologies Clinic “Archi Med”, Panfilovsky prosp., 1205, Moscow, Zelenograd, 124460, Russia.
International Neuropsychiatric Disease Journal, 4 (1), 2015.
1. INTRODUCTION
The number of studies of the last decades were aimed at seeking possible role of neurotropic herpes viruses (herpes simplex of 1 and 2, types, human herpes virus 6 and 8 types, cytomegalovirus, Epstein-Barr virus and varicella zoster virus – HSV-1and 2; HHV-6 and 8; CMV; EBV, HZV) in the pathogenesis of schizophrenia.
In studies of' Leweke et al. [1], Tedla et al. [2] it was shown that the level of IgG to CMV in the blood serum in patients with schizophrenia exceeds that in unaffected controls. Similar differences in IgG to the pointed virus were found in the study of their level in cerebrospinal fluid (CSF) of untreated patients compared with controls without psychiatric diseases (1). Studying the level of Ig to the family of herpes viruses and schizophrenia among military personnel, Niebuchr et al. [3] found a significant association between HSV-6 and schizophrenia; among black there was a significant positive association with HSV 1. A strong trend towards a higher rate of IgG to HSV 1 and 2 has been shown for the schizophrenic group as compared with healthy controls in the investigation of Krause [4]. The patients with schizophrenia had also significantly higher rates of seropositivity to HSV (1 and 2) IgG and CMV IgG than Tourette patients [4]. A higher prevalence of HHV-8 infection in schizophrenic patients than in controls was found by Hannachi et al. [5].
However, the data relating to the content of Ig to herpes viruses in blood serum of patients with schizophrenia are inconsistent. In particular, it was reported that there were no differences between patients with schizophrenia and healthy controls in the level of serum Ig to HSV1, HSV2, EBV [1,2]. Also there were revealed lower levels of Ig G to HSV-6 and HZV in the serum of patients with schizophrenia as compared with controls [1].
The whole series of investigations was performed to study whether exposures to herpes viruses alter cognitive impairment. In several studies [6-10] replicable association of HSV-1 exposure and cognitive impairments in schizophrenia was revealed: The seropositive patients performed significantly worse than seronegative ones on neuropsychological measures of psychomotor speed, executive functioning, and explicit verbal memory. Additionally in Shirts et al. investigation [6] impaired cognitive function (measured by Trail Making Test) in patients with schizophrenia was associated both with HSV-1 and CMV exposure. Morphometric MRI analysis was done in Schretlen et al. [7] investigation to study neuroanatomic abnormalities related to HSV-1 in schizophrenia. It was shown that the reduced grey matter volume in the anterior cingulated and
area of cerebellum distinguish the seropositive patients from seronegative ones. Significant gray matter loss in the posterior cingulated gyrus was noted in the long-time Prasad et al. [8] study among HSV1-seropositive schizophrenia subjects.
Complex mechanisms of herpesviruses impact (together with some other viruses) in pathogenesis of schizophrenia were hypothesized. These mechanisms include both destructive effect of viruses onto the cells with subsequent development of latent inflammatory and degenerative alterations in the tissue of central and peripheral nervous system, and their interaction with DNA, including the integration into genome [11-15].
The possibility of herpes viruses` multiple persistence has been little studied. Also few studies were done to establish correlations between the course of schizophrenia and symptoms peculiarities with exposure to human herpesviruses.
Having studied a small sample of patient with acute schizophrenia (8 subjects), Fukuda et al. [16] revealed no changes in antibody levels to 5 herpes viruses (HSV-1, HSV- 2, HSV-6, EBV, CMV, VZV) during the course of the disease. Dickerson et al. [17] investigated association of serum antibodies to herpes viruses and deficit schizophrenia. Studied patients of the deficit group had significantly more emotional withdrawal, poor rapport, social withdrawal, and poverty of speech; less severe delusions, hallucinations, suspiciousness, and somatic concern as compared with non-deficit ones. Deficit status was significantly associated with the presence of antibodies to CMV. A total 52.3% deficit patients were CMV seropositive, while only 35.3% seropositive cases were revealed among non-deficit group. There was not a significant association between deficit status and antibodies to other herpes viruses tested, including HSV-2, HHV-6, VZV, EBV. Although a univariate association between HSV-1 and deficit status was also established, this association became non-significant in the multinomial logistic regression when including age, gender, age of onset, and hallucinations + delusions. Another study of Dickerson et al. [18], despite the large volume of studied patients with schizophrenia, did not install the effect of HSV-1 exposure on the severity of symptoms measured by the PANS scale.
The investigation of Wang et al. [19] of a large cohort of Dutch adolescents established significant correlation between the serological evidence of Epstein-Barr infection and the severity of subclinical disorders (CAPE scale) only for male patients. Early subclinical manifestation of psychosis, as is known, can be paired with a high risk of developing schizophrenia in later life.
In recent Hannachi et al. investigation [5] that used solid standardized psychopathology measures (PANSS, SANS, SAPS, CGI, BPRS and GAF) among schizophrenic patients, HHV-8 prevalence was statically associated with positive disease symptoms.
There were established significant correlations of Ig М and G levels to HSV- 1, HSV- 2, CMV and EBV with psychiatric symptoms severity measured by the BPRS scale in our preliminary investigation [20]. However, these data need confirmation. Also, there is lack of data about the immunity peculiarities related to the herpes viruses’ persistence in patients with schizophrenia. Considering the above we have assumed that if herpes viruses are among the etiopathogenetic factors of schizophrenia, infection with these viruses should be related to the multiple reactions of the immune system on the introduction or activation of these infects. In turn, these reactions must be associated with the severity of clinical symptoms and their dynamics.
So, our study goal was: To study the relationships of acute episodes of remittent paranoid schizophrenia and herpes virus infection including the analysis of the correlations of clinical symptoms with serum antibody levels and multiparametric immunity characteristics.
2. MATERIALS AND METHODS
Examination of patients was carried out in the “Mental Health” clinic (during 2009 – 2011) in connection with acute exacerbations of schizophrenia or the very first manifestation of the disease. The “Mental Health” clinic is the first Russian private specialized psychiatric clinic operating since 2003. The clinic provides treatment to 200 numbers of primary outpatients each month. It has a small hospital with high comfort conditions for 25 beds.
Patients were initially screened for eligibility on the basis of diagnostic criteria of the acute episode of remittent paranoid schizophrenia according to ICD-10. Clinical psychiatric examination included interview about current state, anamnesis taking, and observations. The final diagnosis of each participant was made by three psychiatrists of high qualification. Another inclusion criterion was the age between 18 and 51. Exclusion criteria were: Substance abuse during; mental retardation; history of encephalitis; head trauma or any other reported neurological disorders of the central nervous system that had resulted in past or current treatment; clinically manifested somatic diseases; clinically apparent herpesvirus infection; recent treatment with antiviral medications.
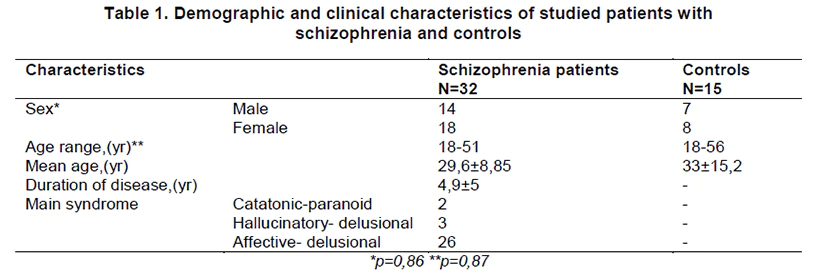
In total, 32 patients with the paranoid schizophrenia (episodic remittent form) (F20.03 by ICD-10) were examined. The age of patients varied from 18 to 51, the patients age 18-33 years being more prevalent (n=25). The average duration of the disease from the moment of its first manifestations in most of cases (18) was not longer than 5 years (Table 1). 30 patients were not receiving psychotropic drugs before admission to the clinic and only 2 were on a regular psychotropic therapy.
The syndromal psychiatric assessment of patients at the time of examination is presented in Table 1. The Brief Psychiatric Rating Scale (BPRS) [21] was used to assess the severity of the psychopathology. The average global assessment of severity of the psychopathological symptoms was 3.4+2.3. The controls included 15 healthy subjects comparable by age and sex (Table 1) without any psychiatric co-morbidities. They were selected among persons that were examined preventively in the Modern Medical Technologies Clinic “ArchiMed”. Exclusion criteria for controls coincided with those for patients.
2.1 Immunological Methods
We determined the leukocyte content, the lymphocyte subpopulations and the leukocyte phagocytosis in «PHAGOTEST» ("EXBIO Praha", Czech Republic) with fluorescein (FITC)- labeled opsonized bacteria and calculated the phagocytic index (PhI), the circulating immune complexes (CIC) level by spectrophotometry. The antibodies to the herpes viruses (HSV-1, HSV-2, CMV, EBV) (both IgG and IgM) were determined using the ELISA test. Total serum immunoglobulins (IgG and IgM as well as IgA), were determined by immunoturbidimetry.
2.2 Statistic Analysis Results were statistically processed using the software package Statistica 6.0 for Windows (StatSoft, USA). The mean (M) and standard deviation (SD) were deduced. For data with normal distribution, inter-group comparisons were performed using Student’s t-test. The Mann-Whitney U -test was used to compare the differences between two independent groups (for nonparametric data). Spearman’s rank correlation coefficient was also used. Pearson’s Correlation Coefficient (r) was used to determine the strength of the relationship between two continuous variables. A value of P<0.05 was considered statistically significant. 3. RESULTS
Analysis of the obtained data revealed the number of regularities describing the studied patients.
It should be noted that most of the population is infected with herpes viruses (80-90% - with HSV- 1 only [22]), and commonly occurs at an early age. Herpes virus never disappears; it persists for lifetime [23]. Actually, virologists consider the presence of IgM itself (in the range of reference values) as a sign of acute infection [24].
Based on the same positions, upon constant presence of a herpesvirus in the body, fluctuations of IgG level to this virus can be considered reflecting the degree of its activity. In connection with abovementioned, the analysis of correlations included absolute values of antibodies levels, not taking into account excess of reference values level.
3. RESULTS
3.1 Analysis of the Multi-parametric Immunity Parameters
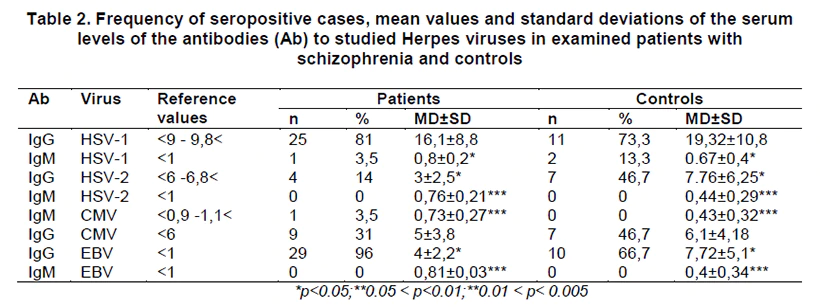
Analysis of specific antiviral resistance revealed in all the patients, except for the 2 patients, a positive reaction for antibodies to any type of herpes viruses (seropositive cases). The reaction was considered positive if the antibody level was greater than the reference value (Table 2).
The maximal number of patients demonstrated the positive reaction for IgG to HSV-1 (81%) and EBV (96%) and, in the least, to CMV (31%). The seropositive to HSV-2 (increased IgG level) were 14% of patients. It is important that although IgM values exceeded the norm only in 2 patients (7%), practically all the parameters (excepting 5 parameters for the total sample) were differing from zero. In the conditions of partial immunodeficiency, characterizing herpetic infection, this data can suggest exacerbation of infectious processes in both groups. Recall that according to virologists’ findings, the levels of the specific IgM antibodies above zero clearly indicate to infectious process induced by the relevant agent [24].
On the other hand, in controls the positive titers of the HSV-1 IgG antibodies were detected in 73,3%, of the VEB IgG antibodies – in 66,7%, of the HSV-2 and CMV IgG antibodies – in 46,7% , of the HSV-1 IgM antibodies - in 13,3%. There were no cases with the positive titers of HSV-2 and CMV IgM antibodies in this group.
The Table 2 data reveals exceeded IgG levels to HSV-1 and especially to EBV in both studied groups. Only Ig M titers (to HSV-1, HSV-2, CMV and EBV) significantly exceeded corresponding titers in patients in comparison with controls. On the contrary, only IgG titers (to HSV-2 and EBV) significantly exceeded corresponding titers in controls in comparison with patients. So, these data identify in patients more active specific humoral immune response to herpetic infection than in controls. It can be supposed that clinically unmanifested infectious process is associated with herpesviruses in controls. This process may be the initial stage of any physical illness.
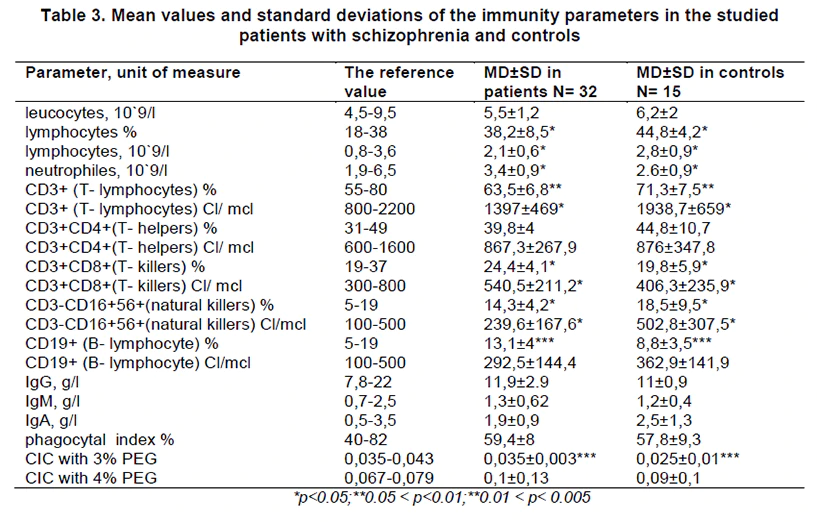
As shown by the study of other parameters of immunity, in both groups there was a significant percentage of persons with a relative limphocytosis (an excess proportion of lymphocytes in leukocyte formula under normal of their absolute content in the blood): 47, 8% patients and 60% controls. These data argue in favor of acute viral infection and taking into account the data of Table 2 suggest herpetic infection.
The data presented in the Table 3 indicate to a greater activity of humoral immunity in patients compared with controls. The marked deviation is a characteristic of the viral, in particular, herpetic infections. It cannot be excluded that differences in the studied immunological parameters are associated with a more protracted nature of infection in patients. In favor of this opinion a higher content of T - killers, B-lymphocyte, CIC with 3% PEG in patients can testify. In contrary, the total number of lymphocytes and natural killers, providing nonspecific resistance, in controls exceeded those in patients. Summarizing the data from the Tables 2 and 3, it can be concluded that the results of multiparametric immunity characteristics investigation in patients with remittent paranoid schizophrenia and controls can indicate to herpetic infection in both studied groups.
3.2 Correlation Analysis of Immunity Characteristics with the Clinical Parameters in the Examined Patients with Remittent Paranoid Schizophrenia
The relationships of the antibody levels to herpes viruses with the type of immune response and some clinical characteristics measured by BPRS in the examined patients with remittent paranoid schizophrenia were revealed. These relationships we presented as clinical-paraclinical complexes. Note that such complexes don’t describe the psychical status of patients in general, being a part of their structure. The identified complexes were conditionally called as «hypochondriac», «affective» and «psychotic».
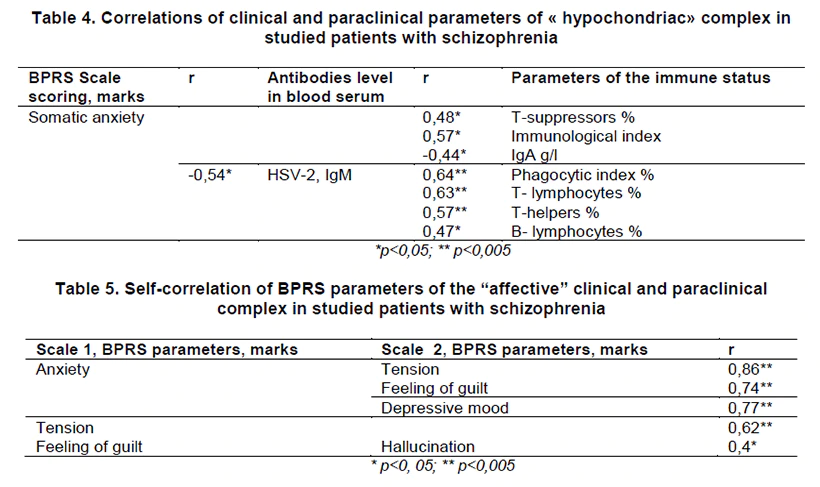
1. The «hypochondriac» complex included only one clinical parameter – «somatic anxiety» (non-delusional level of severity). As seen from the Table 4, such clinical sign as “somatic anxiety” can reflect the unfolded immune reaction to primary infection or reinfection by HSV-2. This fact is supported by the involvement of all of the three types of the immune response (humoral, cellular, phagocyte) in correlations. Taking into account that the negative correlation of the “somatic anxiety” with IgА level reflects the reaction to overcoming of immune barrier on the mucous membrane by antigen, the positive correlation of IgМ level to this virus with the percent ratio of Т-helpers indicates to the increasing intensity of the cellular immune response. The sign “somatic anxiety” itself becomes more severe with reducing level of IgM to HSV-2, that is when the viral load increasing. In general, described complex showed that such clinical indication as “somatic anxiety” is, in the first place, the organism reaction to the antigen but not to the immune response.
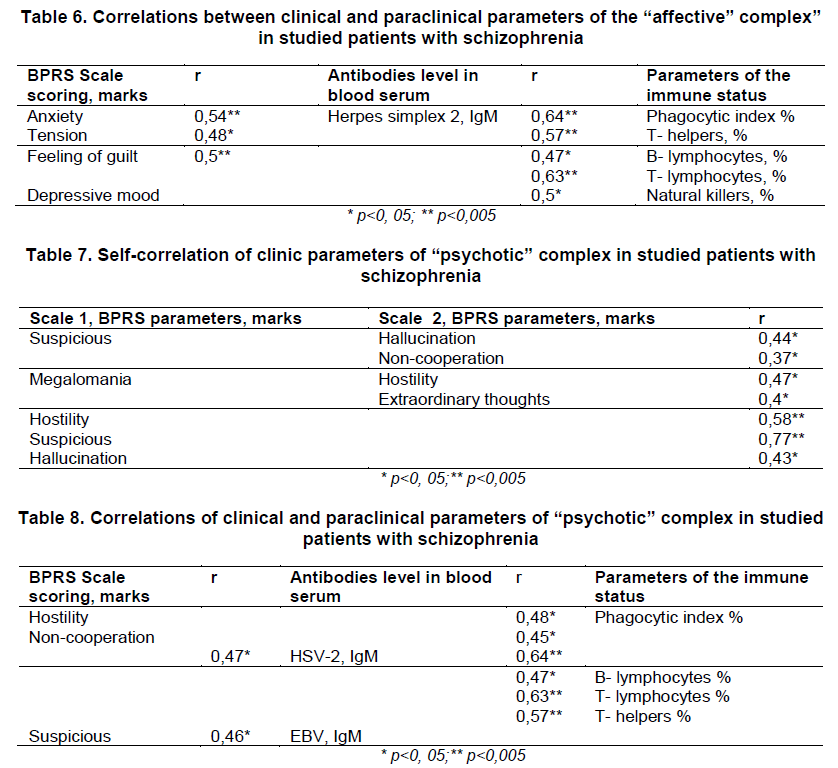
2. The “affective” (anxious-depressive) complex was clinically represented by such correlating BPRS parameters as “anxiety”, “tension”, “depressive mood” and “feeling of guilt”. These clinic symptoms appeared as interrelated not only within themselves, but also with such parameter as hallucination (Table 5). The complex presented in Table 6 reflects the activation of HSV-2 (correlations of the clinical symptoms and IgM level). It is worth noting that the “depressive mood” parameter is related to the reaction of immune system in the form of antibody-independent cytotoxicity (the correlation with natural killers content). Other interrelated symptoms (“anxiety”, “tension”, “feeling of guilt”) reflect the acute and unfolded immune response (the correlations with phagocytic index, content of Т-helpers, В-lymphocytes, Т-lymphocytes). Comparison of the studied complex with the previous one reveals their significant identity by their paraclinical parameters. However, if the clinic parameter “somatic anxiety” is more related to the influence of antigen, then clinical components of the “affective” complex are more related to the immune response itself (direct correlation between clinical symptoms and cellular immunity parameters).
3. The “psychotic” complex includes such correlating clinical parameters as “suspicion”, “hostility” and “non-cooperation” which are related with the other characteristics of paranoid state (Table 7).
The Table 8 shows clinical and paraclinical parameters correlations of the “psychotic” complex. It is seen that the “psychotic” complex develops as acute immune response to activity of HSV-2 and EBV (IgM to both viruses). By accounting to the unfolded reaction of cellular immunity to HSV-2 (the correlations with phagocytic index, content of В-lymphocytes, Т- lymphocytes and Т-helpers) and its absence to EBV one can conclude that course of infectious processes caused by these viruses have the differences. Positive value of correlations represented in the Table allows to state that psychosis symptoms are more related to the immune response to viruses than to their own influence: The severity of symptoms increases with the humoral immune response intensification (Ig M) as well as cellular immune reactions.
4. DISCUSSION
Our investigation revealed in all the patients, except for the 2, a positive reaction for antibodies to any type of herpes viruses (seropositive cases). The maximal number of patients demonstrated the positive reaction for IgG to EBV (96%), HSV-1 (81%) and CMV (31%). The frequency of detection of seropositive to CMV cases among our patients is close to that in patients with non-deficit schizophrenia investigated by Dickenson (35,3%) [17].
As in the study of the Leweke et al. [1], the level of IgG to EBV in our patients did not exceed (and was even below) the same parameter in healthy controls. But a high percentage of seropositive patients, as well as a highly significant excess of IgM to EBV in this group (approaching the upper limit of normal) as compared with controls can suppose the contribution of this virus to the pathogenesis of the disease.
A similar situation is observed with respect to HSV-1. As in other studies [1,2], there were not any significant differences in the level of IgG to HSV-1 between patients and controls. However, a high percentage of seropositive patients, and significant excess of IgM to HSV-1 in this group (approaching the upper limit of normal) in comparison with controls may indicate a possible role of this virus in the development of schizophrenia. The last one was confirmed by studies revealed a replicable relationship of HSV- 1 exposure and cognitive impairments in schizophrenia [6-10]. It should be noted that Krause et al. [4] established a strong trend towards a higher rate of IgG to HSV 1 in patients with schizophrenia as compared with unaffected controls. They also found out that schizophrenic patients had significantly higher rates of seropositivity to HSV1 IgG than Tourette patients.
In some studies, the level of Ig G to CMV in patients with schizophrenia was higher than that in healthy controls [1,2] and patients with other disorders (Tourette syndrome) [4]. In our study, the content of Ig G to CMV in patients with schizophrenia did not significantly differ from that of the controls. However, the level of Ig M to CMV, approaching the upper limit of normal, in patients significantly exceeded this parameter in the controls.
In general only Ig M titers (to HSV-1, HSV-2, CMV and EBV) significantly exceeded corresponding titers in patients in comparison with studied controls. These data identify in patients more active specific humoral immune response to herpetic infection than in controls. This conclusion was confirmed by identification in patients more active links providing specific antiviral resistance (T-killers, B-lymphocyte, CIC with 3% PEG). The pattern of changes of immune parameters in controls differed from that in patients and reflected greater activity of the immunity links providing nonspecific resistance. Taking into account the fact that the level of pointed parameters was, as a rule, in reference values interval in both groups at the presence of herpetic infection (specific IgM in both groups), the data can presumably indicate to slow course of this infection (more protracted in patients).
The level of Ig G to VEB and HSV-2 in our patients was lower compared with that in controls. A similar situation was installed by Leweke et al. [1] in respect of Ig G to HSV-6 and VZV, which level in patients was lower than in controls. We can suggest that this fact is connected with partial immune deficits in schizophrenia.
More detailed data confirming the involvement of herpes viruses in etiopathogenesis of schizophrenia were obtained in this study with additional analysis of multiple relationships of immunity characteristics with clinical symptoms. Works studying polymodal system connections between antibodies to herpes viruses, other immunity parameters and disease symptoms in schizophrenia do not occur practically.
In our study, the level of IgM to HSV-2 was correlated with deployed immune reaction involving the humoral, cellular, and phagocytic immunity and occurrence of clinical symptoms as "somatic concerns" (provisionally designated "hypochondriac" complex). Correlation of the content of Ig M to HSV-2 with immune reaction in the form of antibody-dependent cell-mediated cytotoxicity was associated with deployed anxiety-depressive syndrome ("affective" complex).
Correlation of Ig M to HSV-2 with a comprehensive response of cellular link of the immunity (including phagocytic index, the content of B-lymphocytes, T-lymphocytes, Thelpers) under condition of EBV activation (IgM to this virus) revealed conjugacy with the formation of a psychotic state. Our data confirm the results of previous studies of Wang et al. [19], established that at least in some cases (male patients) psychotic symptoms may correlate with the serological evidence of Epstein-Barr infection.
Thus, the established relationships of the clinical symptoms and immune reactions together with pointed above immune regularity may indicate an acute infectious process caused by HSV-2, with the support of EBV as an important pathogenetic stage of development of psychotic episodes of remittent paranoid schizophrenia. Acute infectious process unfolds in the network of a mixed herpesvirus infection, associated with of HSV-1 and CMV. The last one is outstanding due to significantly higher level of IgM in patients compared with controls for both viruses and high frequency of seropositive cases for HSV-1.
Considering the three described clinical and paraclinical complexes, we can develop a hypothesis about the dynamics of infectious process development and associated clinical symptoms. As it is known, clinical dynamics of the episode is “started” by affective complex of symptoms. At the early stages of depressive states development non-delusional fixation of patient on bodily sensations is possible. Psychotic symptoms occur upon worsening affective disorders.
Dynamics of pathological changes in cellular and tissue structures, in particular, in the nervous tissue cells, in the interaction with a viral agent is unfolded in the direction of engagement of the virus in work of cell receptor apparatus by similarity of its epitopes and epitopes of cellular receptors with subsequent penetration of the virus into cell and impaired synthesis of cellular DNA and RNA [23,25] Virus-infected cells are eliminated in the early stages of the immune response by phagocytes, T-killers of lymphocytes. The increasing complexity and worsening of this process is connected with the influence on the cellular structures of the complexes of antigens - antibodies, starting a cascade of further changes in the tissues, associated with autoimmune processes. These processes were detected in patients with schizophrenia at increased levels of autoantibodies to glutamate receptors [26], GABA and nACh receptors [27], voltage-gated calcium channel [27] and a number of intracellular microstructures of nervous tissue, including glial fibrillary acidic protein, basic myelin protein and specific axons` protein NF- 200 [27]. The relationship of these changes with infectious-inflammatory processes was justified [27].
If we assume that the selected clinical and paraclinical complexes reflect the sequence of brain tissue damage and symptoms associated to it, we will get the data accuracy in both the dynamics line of psychopathological symptoms and the line of immunopathological changes. The first two complexes, reflecting the initial stages of schizophrenia episode (affective disorders, including nondilusional fixation on bodily sensations), reflect the early stages of acute infectious process caused by the HSV-2 and specific dynamics of the immune response. The further development of the clinical picture of the episode is associated with activation of EBV and the emergence of psychotic symptoms. This stage of the episode is related to the activation of autoimmune processes and massive cell death. In this connection it should be mentioned that currently EBV is considered to be involved in many, if not all the autoimmune processes [28].
It should be noted that for initiation of psychotic episode insufficiently active immune response to HSV-2 seems to have significance (as indicated by level of Ig M to HSV-2 not extending beyond the reference values), upon condition of massive latent infection connected with EBV (high level of IgG to EBV in the patients examined). Latent infection connected with other viruses of herpes family especially with HSV-1 (high level of IgG to this virus), reduces immunity and may cause the dimly expressed psychopathological symptoms, being a predisposing factor for manifestation of the disease.
We should mention again that the analysis of the material presented here was performed taking into account that the organism infected with herpes virus will never be released from it, and so-called “healthy carriage” is a non-active phase of infectious process. If not to adhere to these ideas, many of the positions expressed here could be questioned. Nevertheless, there will be a conclusion that antibodies to the herpes family viruses are involved in the pathogenesis of schizophrenia and their level is associated with the severity of symptoms of psychotic episodes, which confirms the results of our preliminary researches [20]. This fact dictates, already at this stage of research, implementation of anti-viral drags together with psychotropic remedies into the therapeutic complexes for the patients with schizophrenia, as well as dynamic control of the antiviral antibodies level.
We must bear in mind that the studied complexes were singled out of the possible broader relationships of clinical and immunological parameters. This may be due to the probabilistic contribution to the development of immunopathological and psychopathological disorders of other microorganisms presented in the microbiota. Earlier, on the basis of lifetime microbiological diagnosis, we reported on microbial associations in patients with schizophrenia associated with the development of acute and chronic pathological processes, and including other microorganisms along with other herpes viruses (adeno-, enteroviruses, influenza viruses, toxoplasma, chlamydia etc. [15]. The possible participation of the mentioned microorganisms in the pathogenesis of schizophrenia was discussed in many other studies [4,12,29-32 et others]. However, the study of relations of the clinical features of cerebral pathology with the role of the herpes viruses as a leading pathogenic neurotrophic human factor remains one of the most important tasks of clinical medicine.
5. CONCLUSION
The research results may indicate an acute infectious process caused by HSV-2, with the support of EBV as an important pathogenetic stage of development of psychotic episodes of remittent paranoid schizophrenia. Acute infectious process unfolds in the network of a mixed herpesvirus infection associated with persistence of CMV and HSV1.
4.1 Limitations of the Study
- we investigated multiple immunological parameters, but not all the possible (for example, interferon, cytokines and others).
- we investigated several herpes viruses, but not all the known (for example HVS-6, VZV).
CONSENT
All authors declare that ‘written informed consents were obtained from the patients for processing survey data.
ETHICAL APPROVAL
This section is not applicable. Examination of the patients was carried out as part of usual diagnostic standards necessary to assess the status of patients and treatment prescription. Surveys of this kind do not require authorization of the Ethics Committees in Russia.
COMPETING INTERESTS
The authors have no conflict of interest with any commercial or other associations in connection with this article.